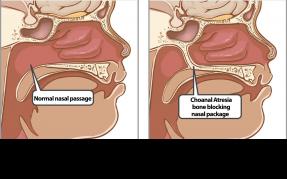
Hydrops fetalis (HF) is a term for the abnormal accumulation of fluid in at least two different fetal compartments. The condition is often characterized by subcutaneous edema, effusions in two or more serous cavities including pericardial or pleural effusions and ascites, with associated polyhydramnios and increased placental thickness.
Hydrops fetalis is most times regarded as a fatal condition and diagnosed following ultrasonography, and in most cases occurs in rhesus alloimmunization especially before prophylactic anti-D administration in the developed countries, although an entirely different scenario may be encountered in the developing nations.
Generally, there are two categories of Hydrops fetalis: isoimmume and nonimmune Hydrops fetalis that develops in the presence of maternal antibody-fetal antigen-mediated red blood cell hemolysis is referred to as isoimmune hydrop fetalis (IHF). Hydrops fetalis that develops in the absence of maternal antibody-fetal antigen-mediated red blood cell hemolysis is classified as nonimmune hydrops fetalis (NIHF). The incidence of isoimmune hydrop fetalis has markedly declined after the use of anti-D gammaglobubin prophylaxis. At present, nonimmune hydrops fetalis accounts for 85-90% of Hydrops fetalis cases.
Non-immune hydrops fetalis is a severe fetal condition defined as the excessive accumulation of fetal fluid within the fetal extravascular compartments and body cavities, including the serous cavities such as pericardial, pleural, and peritoneal, with associated skin oedema.
The prevalence of non-immune hydrops fetalis is unknown as it is difficult to obtain when many cases are not diagnosed before intrauterine death or may spontaneously resolve antenatal. Currently, about 90% of cases of hydrops are non- immune hydrops fetalis, with prevalence reported as 1 in 1,700-3,000 pregnancies.
Non-immune hydrops fetalis are the result of an increase in interstitial fluid production. The causes can be different, such as those cardiovascular which make up about 21.7% (as Ebstein malformation, tetralogy of Fallot), hematologic which represent 10.4% (Hb Bart's HF), chromosomal; 13.4% (Turner syndrome), infectious (parvovirus B19; Toxoplasma gondii; Rubella virus; cytomegalovirus; herpes simplex virus; enterovirus; syphilis; chickenpox virus; Lyme disease), and more rarely: syndromic (Costello syndrome, Meckel syndrome), inborn errors of metabolism (mucopolysaccharidosis, transaldolase deficiency, GM1 gangliosidosis type 1, Niemann-Pick disease type C), urinary and thoracic tract malformations, and congenital diaphragmatic hernia or idiopathic.
This is the most serious form of Rh hemolytic disease (HDFN). Excessive destruction of the fetal red cells leads to severe anemia, tissue anoxemia and metabolic acidosis. These have adverse effects on the fetal heart and brain and on the placenta. Hyperplasia of the placental tissue occurs in an effort to increase the transfer of oxygen but the available fetal red cells (oxygen carrying cells) are progressively diminished due to hemolysis. As a result of fetal anoxemia, there is damage to the liver leading to hypoproteinemia which is responsible for generalized edema (hydrops fetalis), ascites and hydrothorax. Fetal death occurs sooner or later due to cardiac failure. The baby is either stillborn or macerated and even if born alive, dies soon after.
The following are the diagnostic features: (1) mother is Rh-negative; (2) serological examination reveals presence of Rh-antibody; (3) there may be presence of polyhydramnios; (4) previous history of affection of a baby due to hemolytic disease; (5) sonography-(real time combined with pulse Doppler) to detect edema in the skin, scalp and pleural or pericardial effusion and echogenic bowel; (6) straight X-ray abdomen showing: Buddha position of the fetus with a halo around the head due to edematous scalp; (7) the baby at birth looks pale and edematous with an enlarged abdomen due to ascites. There is enlargement of liver and spleen and (8) placenta is large, pale and edematous with fluid oozing from it. The placental weight may be increased to about half or even almost equal to the fetal weight.
To prevent active immunization of Rh-negative yet unimmunized, Rh anti-D immunoglobulin (IgG) is administered intramuscularly to the mother following childbirth. Mode of action is antibody-mediated immune suppression (AMIS). The anti-D antibody when injected, blocks the Rh-antigen of the fetal cells; the intact antibody coated fetal red cells are removed from the maternal circulation by the spleen or lymph nodes; the fetal red cells, coated with anti D antibodies interfere with the production of IgG from the B cells. It should be administered within 72 hours or preferably earlier following delivery or abortion. It should be given provided the baby born is Rh-positive and the direct Coombs’ test is negative. In case, where the specified time limit is over (>72 hours), she may be given up to 14–28 days after delivery to avoid sensitization. Similarly, when the Rh factor of the fetus cannot be determined, it should be administered without any harm. Anti D-gammaglobulin is administered intramuscularly to the mother 300 µg following delivery. All Rh-negative unsensitized women should receive 50 µg of Rh-immune globulin intramuscular within 72 hours of induced or spontaneous abortion, ectopic or molar pregnancy or CVS in the first trimester. Women with pregnancy beyond 12 weeks should have full dose of 300 µg. Generally 300 µg dose will protect a woman from fetal hemorrhage of upto 30 mL of fetal whole blood.